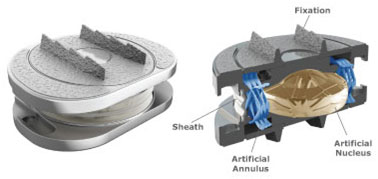
Lumbar Arthroplasty
After first being attempted by Fernstromin the late 1950s, the initial results were promising However, long-term failure of the device attributed to the excessive compressive load into the bone resulted in subsidence and failure of the implant. In the early 1980s, Schellnack and Buttner-Janz revived the concept of an artificial disc with the design of the commercially distributed Charité™ disc. Since then, there has been numerous artificial disc devices approved for use by the FDA, although the number of implants used by surgeons have seen a rapid rise and a rapid fall, and now has plateauedin its usage.
Lumbar arthroplasty is NOT a direct substitute for lumbar fusions.
There are a number of contraindications to the implantation of artificial lumbar disc devices:
- Presence of advanced degeneration
- Previous posterior lumbar surgery
- Previous abdominal/pelvic surgery
- Significant vascular disease
- Advanced age (>50-55)
- Instability and deformity
- Rheumatoid arthritis
- Pregnancy
- Morbid obesity
- Significant osteoporosis
- Cancer related spinal conditions
- Allergies to stainless steel/cobalt-chrome.
Procedure
The surgery is performed general anaesthesia. You will lie on the operating table faced up, and the abdomen is draped in a sterile fashion. The approach may be performed by your Spine surgeon or a Vascular surgeon. The operation does not require any muscle to be disconnected. A5-8 cm skin incision is made in the anterior abdominal wall. Meticulous dissection behind the muscle layer along the avascular gap allows access to the anterior surface of the lumbar spine. An Xray is performed on the operating table to identify the correct disc space. The blood vessels that lead to your legs will be retracted and protected during the surgery. The disc is completely removed and the bony surface is meticulously prepared to achieve unrestricted contact with the arthroplasty device. At the spinal canal where the spinal cord and exiting nerves are, any bone spurs (osteophytes) and disc fragments must be removed to decompress the important structures.
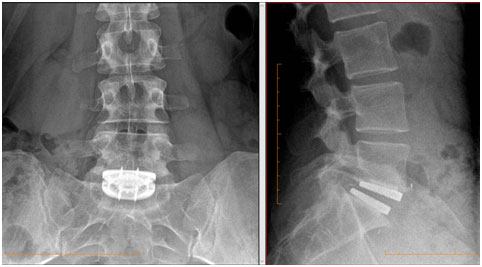
Under Xray guidance, an optimally sized arthroplasty device is inserted in the midline as far posterior as possible into the disc space to maintain the height of the disc space, the natural curve and motion of the lumbar spine.
Risks or Complications
All surgeries carry risk and it is important to understand the risks of the procedure in order to make an informed decision to go ahead with the surgery. In addition to the anaesthetic complications, spinal surgery is associated with some potential risks but not limited to:
- Implant failure/migration
- Poor positioning of implant
- Transient/Long term Nerve injury
- Transient/Long term Spinal cord injury
- Vascular injury
- Kidney and bowel injury
- · Retrograde ejaculation for men
- DVT
- Persistent nerve pain, numbness, tingling, burning, aching
- Persistent abdominal wall andback pain
- Infection
- Postoperative hematoma (bleeding)
- Numbness along the incision site
Benefits
- Motion preservation
- Risk of adjacent (neighbouring) disc degeneration is reduced compared to lumbar fusion
- Less muscle dissection
- Less painful than posterior approaches
- Less bleeding
- Shorter recovery period